
Babaji
NSQ 2, November 2003
Editor:
G Narenthiran, BSc(MedSci), MB ChB (Aberd.), MRCS(Edin.), Senior
SHO, Hull Royal Infirmary, Hull UK
E-mail: g_narenthiran@hotmail.com
Acknowledgements:
Mr Paul Fewings (Hull, UK), Mr Rodney JC Laing (Cambridge, UK), Prof AD Mendelow
(Newcastle, UK), Mr Gerry O'Reilly (Hull, UK), Dr James T Rutka (Toronto, Canada),
Prof Walter R Timperley (Sheffield, UK), Prof Joachim Weis (Bern, Switzerland)
1. The incidence of late post traumatic seizures is reduced
by prophylactic use of phenytoin:
2. In persistent vegetative state brainstem functions are not
preserved:
3. In testing the caloric reflex in an unconscious patient who has preserved brainstem function, irrigation of the external auditory canal with cold water causes deviation of the eyes to the side of irrigation:
4. Gasserian rhyzolysis does not require transversing the subarachnoid space:
5. In the International
subarachnoid aneurysm trial (ISAT) the 30.6% patients allocated for
craniotomy and clipping of aneurysmal neck were disabled or dead compared to
23.7% of the patients who had undergone endovascular treatment with detachable
platinum coils at 1 year:
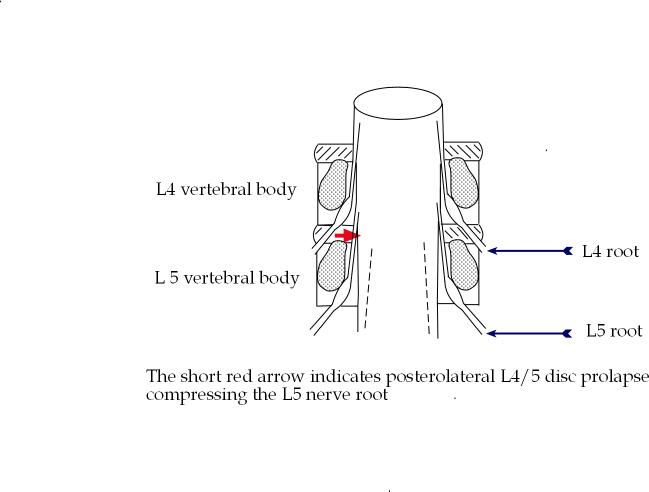
6. Posterolateral L4/5
disc prolapse commonly presents with symptoms and signs corresponding
to L4 radiculopathy::
7. In Gerstmann's
syndrome there is unilateral asomatognosia:
8. Dexamethasone
has 4 times the mineralocorticoid activity as hydrocotisone:
9
. (with
permission from Prof
Walter R Timperley, Sheffield, UK)
(with
permission from Prof
Walter R Timperley, Sheffield, UK)
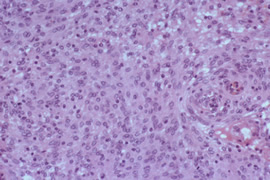
The slide is of vestibular schwannoma:
10.
 (with
permission from Dr J Rutka (Hoffman slide collection)
(with
permission from Dr J Rutka (Hoffman slide collection)
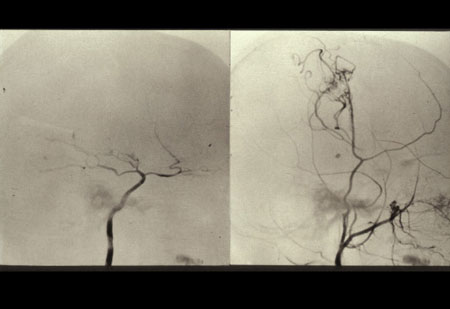
These are angiographic images of Moya Moya disease:
The incidence
of early post-traumatic seizures (within 7days of injury) is reduced by prophylactic
use of phenytoin However, prophylactic use of phenytoin has no beneficial effect
on the late post-traumatic seizures or mortality following severe head injury.
Temkin, N. R., Dikmen, S. S., Wilensky, A. J., et al. A randomized, double-blind
study of phenytoin for the prevention of post-traumatic seizures. N.
Engl. J. Med., 1990; 323:497–502
Haltiner
AM, Newell DW, Temkin NR., et al: Side effects and mortality associated with
use of phenytoin for early posttraumatic seizure prophylaxis. J
Neurosurg., 1999; 91: 588-592
A2. False
In persistent vegetative state there is preservation of complete or partial
brainstem functions: the patient is able to spontaneously breathe and maintain
blood pressure. The patient also has a partial or complete preservation of hypothalamic
functions.
The persistent vegetative state is characterized by a combination of periods
of wakefulness (preservation of sleep-wakefulness cycle) without evidence of
a working mind. (patients can be in persistent vegetative state without having
periods of wakefulness: e.g. if there is bilateral CN III palsy as well from
the original injury).
Jennett B. The vegetative state medical facts, ethical and legal dilemmas. Cambridge:
Cambridge University Press; 2002.
A3. True
There is no nystagmus on 'caloric reflex' testing in an unconscious patient.
However if the brainstem function is intact then the eyes will deviate to the
side of the ear which was irrigated with the cold water (30°C). On irrigation
with warm water (44°C) water the eyes will deviate towards the contralateral
side. There will be no response to caloric reflex testing when there is brainstem
death.
Victor M, Ropper AH..Coma and related disorders of consciousness.
Adams & Victor's Principles of Neurology. 7th ed. McGraw-Hill, New York,
2001 Chapter 17 p380
Gasserian rhyzolysis involves entering the gasserian ganglion anteriorly. It is the posterior part of the ganglion that lies within the subarachnoid space in the Meckel's cave.
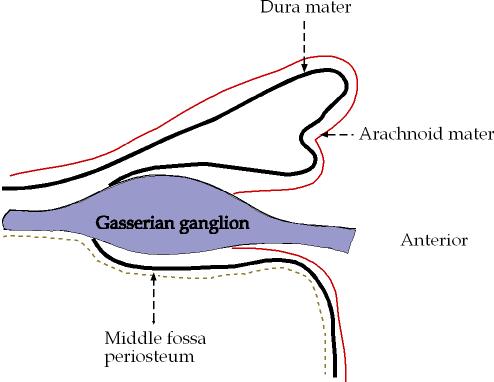
Figure 1. The relationship of gasserian ganglion to dura mater and arachnoid mater
Sinnatamby CS. Last's Anatomy Regional an Applied. 7 ed. Edinburgh: Churchill Livingstone; 1999.
ISAT is an excellent study. It was a randomised prospective study with large number of patients enrolled (2143). However criticisms of the study include:
Multi-centre study involving many neurosurgeons and neuroradiologists. The expertise of the practitioners are not likely to be identical; the study did not compare the best neurosurgery practice against the best endovascular practice.
In ISAT only patients who were considered suitable for either endovascular or neurosurgical treatment were included in the study. Therefore which patients to include in the study would have varied from centre-to-centre depending on the practice and experience of neurosurgeons and neuroradiologists at different centres.
The follow-up period was short: 1 year.
The contributors to the study were primarily from UK and and from continental Europe. The neurosurgical operations would have been performed by accredited neurosurgeons. However, a proportion of these surgeons might not be subspecialised in neurovascular surgery. In North America aneurysmal clipping are often undertaken by sub-specialists in neurovascular surgery. Therefore the findings from ISAT may not necessarily apply to the practice in North America
One of the principal investigators had consulting and advisor agreements (and stock options) with 2 companies manufacturing equipments for neurovascular procedures.
Molyneux
A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, Holman R; International
Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid
Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling
in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet.
2002 Oct 26;360(9342):1267-74.
Posterolateral L4/5 disc prolapse commonly presents with symptoms and signs corresponding to L5 radiculopathy.
Wilkins R.
Lumbar intervertebral disc herniation. In: Rengachary SS WR, editor. Principles
of Neurosurgery. London: Mosby-Wilfe; 1994. p. 45-45.9.
A7. False
In Gerstmann's syndrome there is bilateral asomatognosia (asomatognosia = inability recognise part of one' body). The characteristic features of Gerstmann's syndrome are: finger agnosia, confusion of right and left sides of the body, acalculia and agraphia. Gerstmann syndrome is associated with lesion in the dominant parietal lobe.
Victor M RA. Adams & Victor's Principles of Neurology. 7 ed. New York: McGraw-Hill; 2001.
Mineralocorticoid activity leads to retention of Sodium and water in the kidney. Dexamethasone has almost no mineralocorticoid activity and therefore preferred where water retension is to be avoided e.g vasogenic oedema surrounding cerebral metastasis.
Prednisolone and aldosterone (i.v) have 0.8 and 1000 times the mineralocorticoid activity as hydrocortisone respectively.
Titter JM LL, Mant TGK. A textbook of clinical pharmacology. Fourth ed. London: Arnold; 1999.
It is of meningothelial meningioma with sheets of endothelial cells with little evidence of whorl formation.
On catheter cerebral angiogram in patients with Moya Moya disease the abnormal vessels typically resemble a 'puff of smoke' in appearence. (Moya Moya in Japanes denotes: 'something hazy, like a puff of cigarette smoke drifting in the air')
Neurosurgery Quiz © Annals of Neurosurgery, 2003